Brainstorm: Extracorporeal Liver Support
The purpose of this post is to start a general discussion around the idea of using ultrathin silicon-based membranes and graphene oxide to improve Extracorporeal Liver Support, also called Artificial Liver Support (ALS) for patients with acute liver failure (ALF).
What is Extracorporeal Liver Support?
This is essentially the equivalent of renal dialysis for the liver. One of the major goals if not the primary goal of renal dialysis is to remove water soluble toxins from the blood (i.e. urea, creatinine, beta-2 micro globulin and other middle-weight proteins). In patients with ALF, they also need albumin- or protein-bound toxins to be removed from the blood including bilirubin, bile acids, aromatic amino acids (tryptophan), free fatty acids, etc.
Glossary or Terminology for Blood Purification Techniques [1]:
- 1. Plasmapheresis or plasma exchange: Separation of plasma by the centrifugation method or via membrane filtration facilitates a nonselective removal of all noncellular components of blood.
- 2. Plasma fractionation: Filtration of plasma through very high-permeability membranes (molecular weight cut-off of >70–100 kDa); removes high-molecular-weight substances.
- 3. Hemofiltration: Filtration through medium- to high-permeability membranes (molecular weight cut-off between 15 and 70 kDa).
- 4. Hemodialysis: Removal of water-soluble, low-molecular-weight substances by diffusion across a low-permeability membrane.
- 5. Albumin dialysis or aided transfer: Albumin in the dialysate or bound to the filter membrane enhances the clearance of albumin-bound toxins.
- 6. Adsorption: Circulating blood over a sorbent material like charcoal, neutral resin, or anion-exchange resin removes protein-bound toxins.
For ALS, techniques 2-6 are used, but not necessarily all in the same device or system.
There are two primary ALS commercial systems on the market, sold by the two leaders in hemodialysis. MARS (molecular adsorbent recirculating system) is sold by Gambro and the Prometheus system is sold by Fresenius [1]:
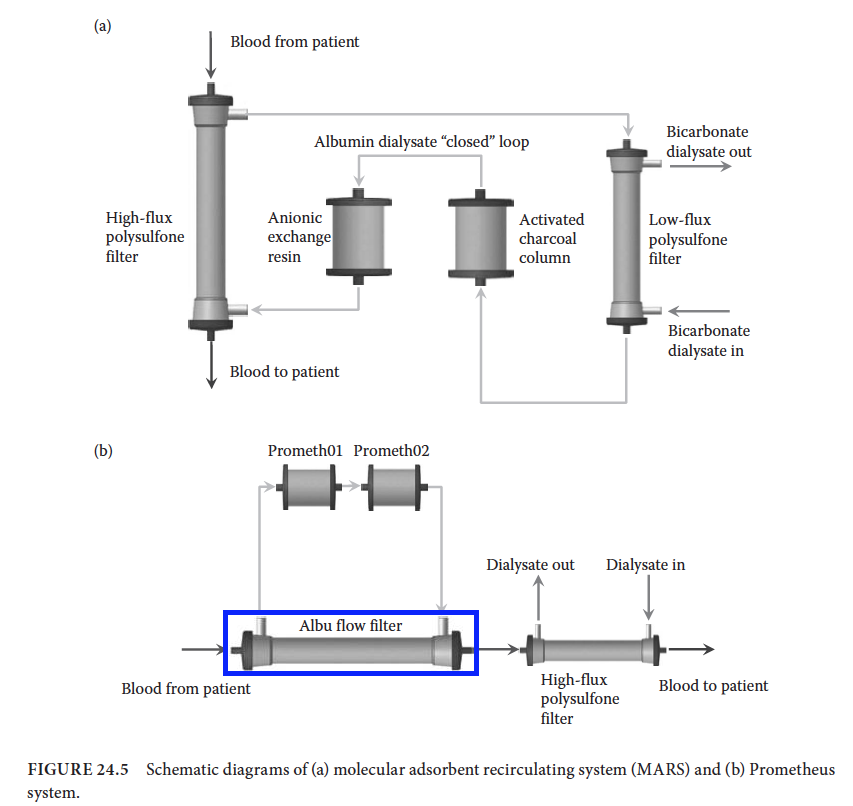
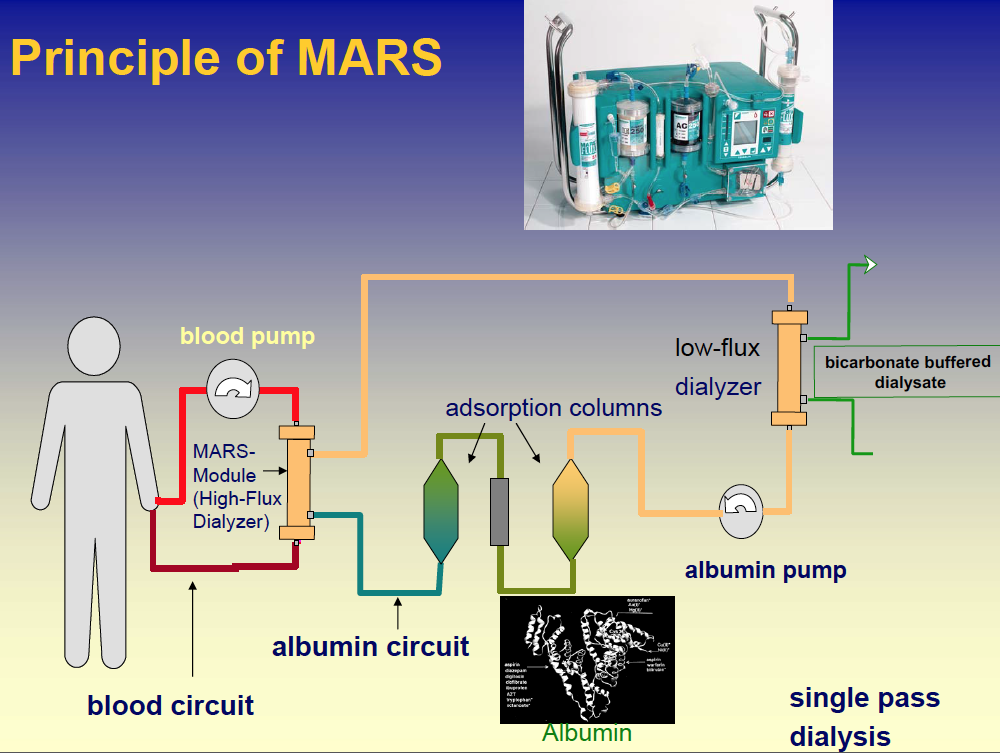
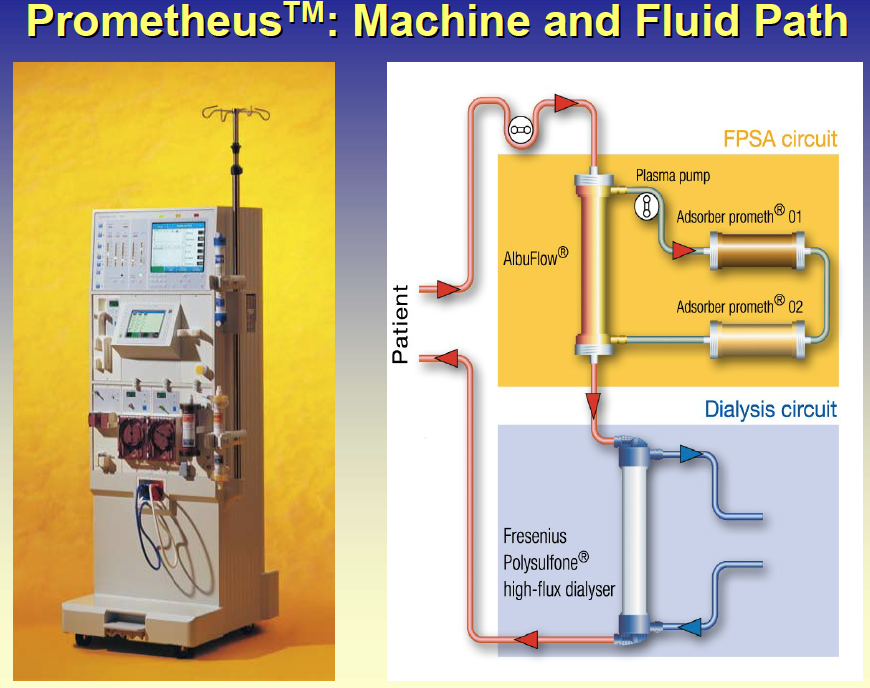
These systems operate very differently. In MARS, the dialysate is rich with albumin and the albumin-bound toxins diffuse or are shuttled across the membrane. The toxins are then cleared from the recirculating albumin dialysate with two adsorbent columns. In the Prometheus system, the blood albumin can pass across a relatively large pore size Albu-flow filter. The blood albumin is cleared of toxins with similar adsorbent columns and returned to the bloodstream. The following schematics are little simpler to follow (from this presentation [2]):

Estimated Market Data [2]:

How can we improve upon these technologies?
Interestingly, there seems to be a lot of debate on the effectiveness and value of these commercial systems. There are several papers that state that the MARS system may reduce bilirubin levels, but does not improve patient survival. Is this the membrane at fault? Is the adsorbent column? Both?
- We could create a thinner more efficient albumin permeable membrane for the Prometheus system using large-pore size NPN.
- The limiting factor in transport in the MARS system is diffusion of protein-bound toxins across the membrane. We could fill the pores or coat the surface of NPN with a lipophilic moiety.
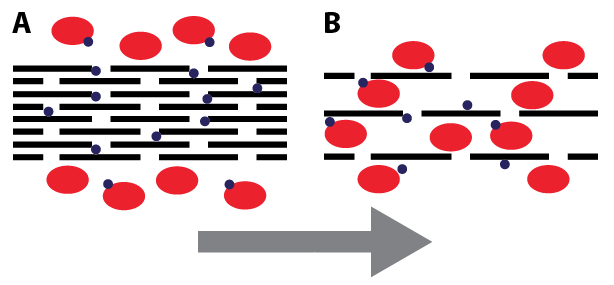
- I am currently “collaborating” with a graphene oxide researcher at the University of Florida. He can create stacks of graphene oxide with very well defined inter-leaflet spacing. In some embodiments, this stack could just act as a typical adsorbent column (spacing ~ 1 nm); with greater spacing (>= 10 nm) toxin-loaded albumin could pass or diffuse through the graphene oxide stack. Due to the thinness of graphene, it has the highest possible surface area to volume and should dramatically improve adsorption. Graphene oxide is also easily chemically modified with standard surface chemistry modifications.

Even though Gambro and Fresenius appear to dominate both the renal dialysis and artificial liver support markets, there is significant research into improving these systems. This Nature Reviews article [3], outlines research on both conventional artificial support systems and bioartificial support systems that are incorporating hepatocytes.
[1] Biomedical Technology and Devices, Chapter 24: Blood-Filtering-Technologies
[2] Artificial Liver Presentation, D. Falkenhagen, Danube University Krems, Artificial-Liver-Background
[3] Nature Reviews article on Artificial Liver Support and Bioartificial Liver Support, Liver_support_strategies-2014
Unsurprisingly, perhaps, the most interesting thing about this to me is the inclusion of albumin in the dialysate. Albumin clearance is not an issue in traditional hemodialysis (or, so conventional wisdom would have you believe) so no such approach is used in renal replacement therapy. Our membranes might change that… So thanks for the literature search terms!
In terms of actual liver dialysis, I think we could make significant strides on clearance; however, as we learned from ECMO, a significant portion of the benefit we see in hemodialysis over traditional techniques is due to the transition from infrequent to continuous treatment. Are patients on liver dialysis on continuous, intensive-care-type support?
I’ll begin thinking about this more. Could be a great perk of our growing body of experience in renal replacement.
We discussed some of this during NRG – so I’ll summarize so we have a written record.
Most patients on ALS have acute liver failure (ALF). They are typically on ALS for a short period of time – as few as 3 sessions of 6-8 hours, sometimes up to 10 sessions over 1-4 weeks. This is because the liver will regenerate and function will recover relatively quickly in many cases (illness, drug overdose, etc.). In cases where the liver is beyond recovery, ALS can be used as a bridge to liver transplant. I think I recall this being more common in Europe than the US. This may be due to the fact that several studies have shown minimal improvement in patient survival with the commercial solutions even though they show reduced bilirubin.