Hemodialysis Vascular Access: Taking the Next Steps (Notes)
Here are the Vascular Interviews in comma separated value form if you want to download them. Here is what I learned or had reinforced.
An arteriovenous fistula (AVF) is the preferred method for creating an easily cannulated access point to large volumetric blood flow for hemodialysis. Normally the distal end of an artery in the arm (e.g. brachial or radial) is dissected and sutured to a nearby vein or a vein which has been transposed. There are more complicated version involving veno-venous anastomosis but they all lead to an AVF which due to pressure will increase in diameter (6 mm is ideal) and provide high blood flow (>600 mL/min) as well as enough length to provide cannulation locations.
Options for vascular access are AVF, arteriovenous graft (AVG), central venous catheter (CVC). (with a fourth option below…)
68% AVF, 18% AVG, 14% CVC in the US, which represents an increase in AVF in the last decades. Training is still behind that of many European countries.
Ideally the AVF should be placed one year before the start of dialysis so it has time to mature and become stable. Predicting who whill need HD and when they will start is problematic. In addition, 60% of attempted arteriovenous fistulas (AVFs) fail. Even with remediation. There has been a lot of work on identifying predictive metrics for AVF maturation success. Some metrics studied to predict success are… Preexisting pathology of the vessels, intimal hyperplasia (thickening of the inner vessel walls), pre-op vascular function tests have not been found predictive in any way. Diameter, flow, and depth (pre-op, and post-op) are the only predictors found so far and these are not reliable. The conclusion from the discussions was that more multi-facility studies need to be conducted to develop predictive tools based on depth of the vessels, flow rate, and vessel diameter.
FDA: The conclusion I came to from the talk from Brian Pullin (Chief of Vascular Surgical Devices) was that early contact with the FDA is best and he directed us to this Device Advice website.
There was also an interesting talk on wall sheer stress (WSS) and its affects on AVF stenosis. Physiological levels of WSS are 10 to 20 dynes/cm2. This is an oscillating flow rather than a steady flow. Mario Remuzzi from the Mario Negri Institute used several COMSOL models to show the WSS throughout the AVF. He also reported findings of increased Nitric Oxide synthesis by the endothelial cells for periodic flow versus laminal flow (turbulent flow restricted the synthesis). Nitric Oxide synthesis is important to combat vascular disease and periodic non-turbulant flow needs to be maintained throughout the AVF to prevent stenosis.
There was an interesting poster by Stephen R. Ash MD of Indiana University Health Arnett and Ash Technology, Inc., Lafayette Indiana. In their approach, which has been tested in one animal. This blood access method inserts an artificial end-to-side anastomosis device into each femoral vein. Plastic tubes with valves lead to ports at the skin surface. Blood flow is 250 to 350 mL/min. One benefit of this is the small amount of foreign material in the vein (the anastomosis like Optiflow, or InterGraft) but you end up with a potential source of infection at the skin. This would not be useful for a pumpless system as the pressure drop between the two veins would be ideally zero.
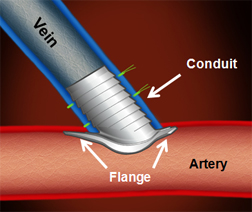 There was a talk by the Optiflow developers. This is a small device made from anti-coagultion plastic and is the essence of a t-intersection. there is a tube structure terminating perpendicularly to to curved flange. The flange resides inside the vessel with the tube protruding through a small opening in the vessel wall. This tube could be connected to the distal end of a dissected artery as in an AVF or a plastic tube as in the above venous access. In the standard use shown in the image, the entire device resides within the vasculature but it is still a small area of foreign material.
There was a talk by the Optiflow developers. This is a small device made from anti-coagultion plastic and is the essence of a t-intersection. there is a tube structure terminating perpendicularly to to curved flange. The flange resides inside the vessel with the tube protruding through a small opening in the vessel wall. This tube could be connected to the distal end of a dissected artery as in an AVF or a plastic tube as in the above venous access. In the standard use shown in the image, the entire device resides within the vasculature but it is still a small area of foreign material.
Not every patient is a good candidate for AVF, some would do better with an AVG, or even a CVC. If our devices use one of these then we have the same problems everyone else has. If we use a modified or a novel access method then we need to be sure we don’t limit our patient pool too much. We don’t want a method that is not useful in obese patients, for example.