Rotation Project Complete: Dialysis of cytochrome c across a commercial membrane
Dan Steiner
Rotation Summary
Abstract
The purpose of this rotation project was to develop and test a clampable system for eventual use in scalable nanomembrane dialysis systems. The nanomembrane dialysis system will be miniaturized into a compact, wearable hemodialysis device that will provide more effective human dialysis treatment (Johnson et al. 2013). For initial tests, a 35 ml reservoir solution containing 1mg/ml of cytochrome c in PBS buffer (Sigma-Aldritch, C2506-250MG) was dialyzed across a 30nm pore size PES commercial membrane (Sartorius-Stedium Biotech, Gottingen, Germany) using PBS as the dialysate solution. Cytochrome c has a native folded radius of gyration of ~1.3nm (Akiyama et al). Cytochrome c concentrations remained at 1.0 +/- 0.03 mg/ml.
Background
Chronic kidney diseases is defined by decreased kidney function over time. End-stage kidney failure results when a patient’s kidneys are unable to provide adequate blood filtration. The predominant treatment method is transplantation, however, the recipient waiting list is far longer than the number of willing donors. This results in patients relying on hemodialysis treatments in order to live with renal failure while waiting for an appropriate donor match (United States Renal Data System).
Hemodialysis is the process by which a machine is used to filter blood extracorporeally. This process is invasive and requires treatment sessions lasting 4 hours as many as 3 times a week. Current machines are often large and require significant training before use (niddk). We believe that miniaturization of the dialyzer, the filter membrane component that facilitates diffusion of salts, urea, and other materials, will lead to compact, wearable devices that will have minimal impact on patient lifestyle, decreased mortality and overall quality of life.

Fig 1. A traditional hemodialyzer https://www.niddk.nih.gov.
The National Institute of Diabetes and Digestive and Kidney Diseases Statistics and facts (Taken directly from: https://www.niddk.nih.gov.).
- The overall prevalence of CKD in the general population is approximately 14 percent.
- High blood pressure and diabetes are the main causes of CKD. Almost half of individuals with CKD also have diabetes and/or self-reported cardiovascular disease (CVD).
- More than 661,000 Americans have kidney failure. Of these, 468,000 individuals are on dialysis, and roughly 193,000 live with a functioning kidney transplant.
- Kidney disease often has no symptoms in its early stages and can go undetected until it is very advanced. (For this reason, kidney disease is often referred to as a “silent disease.”)
- The adjusted incidence rate of ESRD in the United States rose sharply in the 1980s and 1990s, leveled off in the early 2000s, and has declined slightly since its peak in 2006.
- Compared to Caucasians, ESRD prevalence is about 3.7 times greater in African Americans, 1.4 times greater in Native Americans, and 1.5 times greater in Asian Americans.
- Each year, kidney disease kills more people than breast or prostate cancer. In 2013, more than 47,000 Americans died from kidney disease.
Experimental Design
Device design began by machining two polycarbonate blocks (7.2 cm x 7.2 cm x 1.9 cm) with one block having threaded holes (#10) drilled for clamping the PDMS chamber, membrane, and gaskets. The PDMS chamber was cast using the standard 10:1 polymerization ratio and molds that were created by Dr. Dean Johnson. 300 and 100 um silicon gaskets were used to provide the interface between chamber and the membrane. Dr. Johnson also provided silicon gasket dimensions. The device layers were as follows;
| Non-threaded polyacrylamide block |
| PDMS top chamber |
| 300 um small gasket window, thick plastic backing facing PDMS |
| 300 um small gasket window with support struts |
| 100 um large collar surrounding Sartorius commercial membrane |
| 300 um small gasket window with support struts |
| 300 um small gasket window, thick plastic backing facing PDMS |
| PDMS bottom chamber |
| Threaded polyacrylamide blocked |
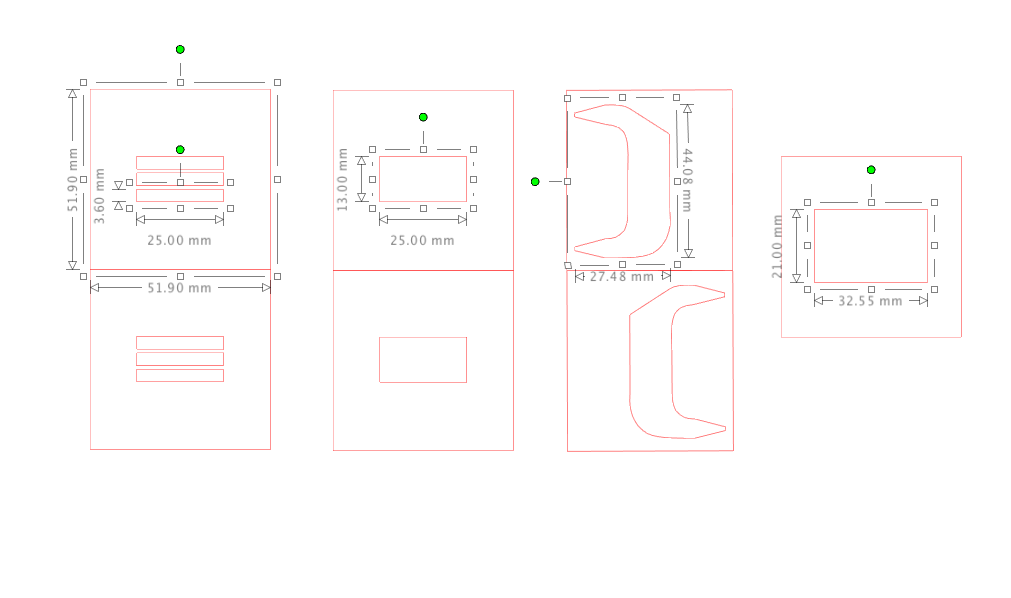
Fig 2. Gasket types and dimensions, along with an outline of the mold dimensions.
Gaskets that were in directed contact with one another were bonded to ease assembly, except for one of the two layers that was adjacent to the membrane. The Sartorius membrane was activated for 1 hour in DH2O, then placed with the dialyzing surface face up towards the reservoir flow surface. 22 Ga needles were inserted into the PDMS to contact the inner chamber. Unpolymerized PDMS was used to seal needle entry ports.
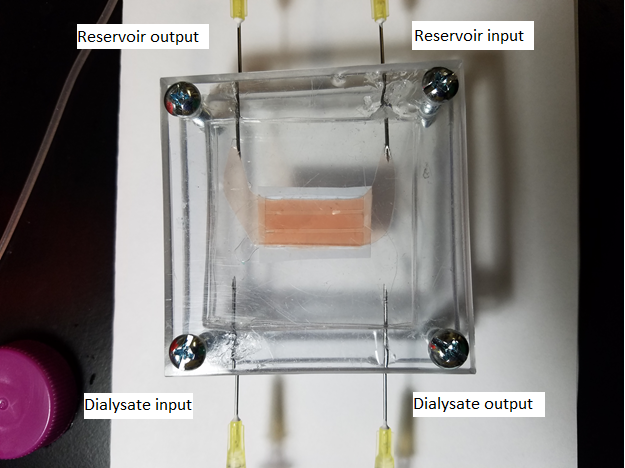
Fig 3. Dialyzer Assembly.
Phosphate buffered saline was used as the cytochrome c sovent and as the dialysate solution (0.8% NaCl, 0.02% KCl, 0.144% Na2HPO4, 0.024% KH2PO4, pH 7.4)
Fluidic system was assembled as per previously posted schematic. The system was primed for 20 minutes using a two-step process, first with 70% isopropyl alcohol followed by DH2O. The two pumps used were a Cole-Parmer mini-pump variable flow 73160-31 and a Cole-Parmer mini-pump variable flow 70730-62. Pump settings were set as optimized by Yorimitsu et al.
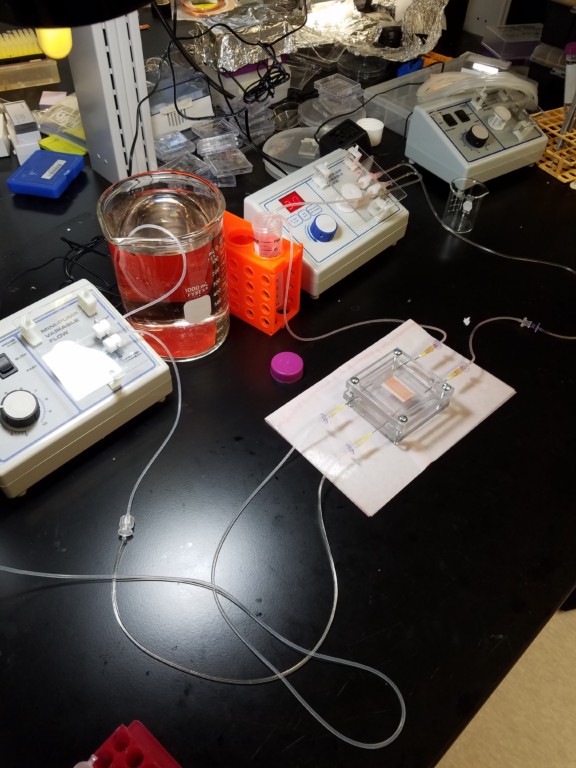
Fig 4. Fluidic System
Table 1. Peristaltic pump settings.
| Model Number | Tubing Size (mm) | Setting | Flow Rate (ml/min) |
| 73160-31 | 6.4 | 30 | 1ml/min |
| 70730-62 | 1.6 | 3 – Slow | 5ml/min |
600 ul fractions were collected every 30 minutes for 4 hours from both the reservoir and the waste dialysate solutions.
Data was collected using a Tecan Infinite M200 Plate Reader. Standard curve data was generated using 0-100% mg/ml cytochrome c from the original stock solution. Data was collected at wavelengths 405-550nm, with 405nm being the accepted wave length from Dr. Johnson’s previous research.
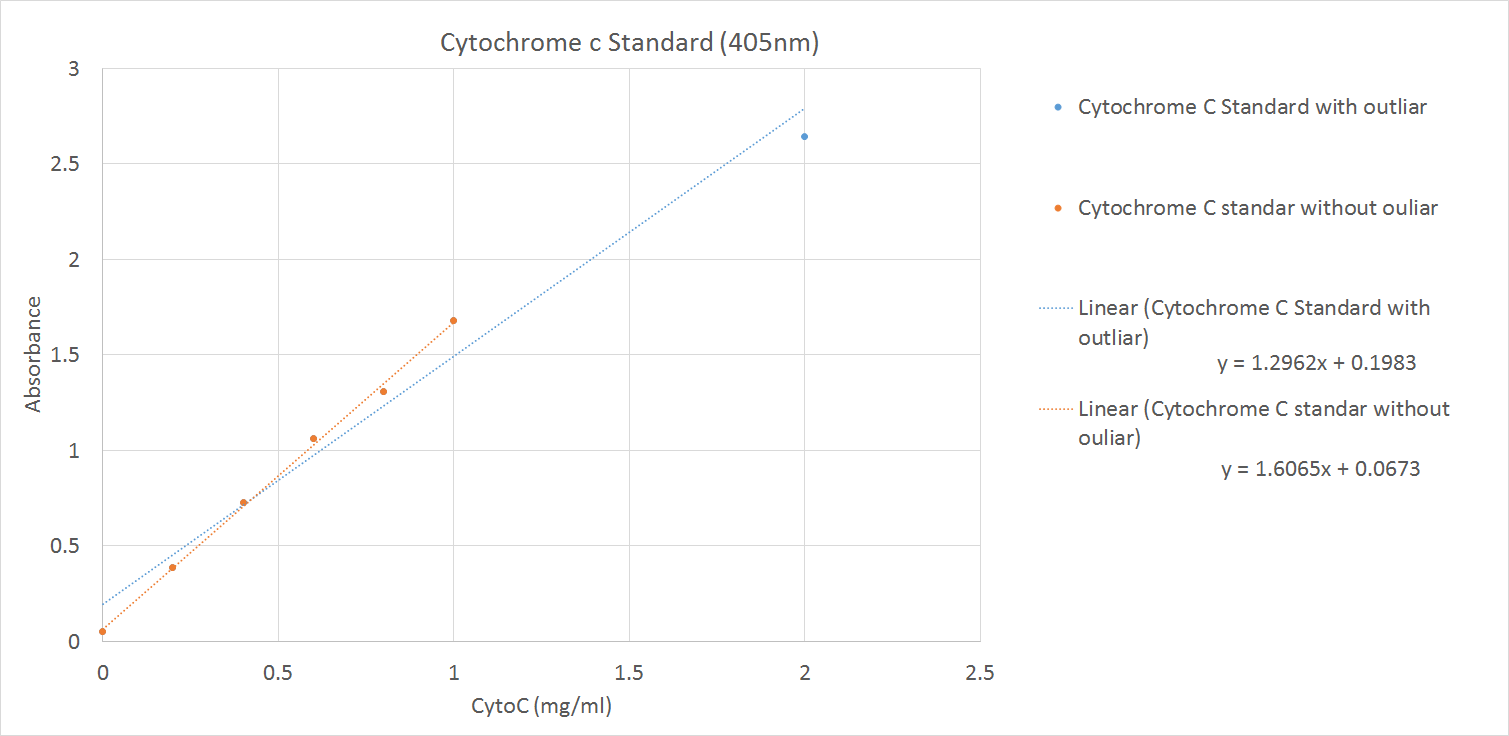
Fig 5. Standard curve for concentrations up to 2 mg/ml.
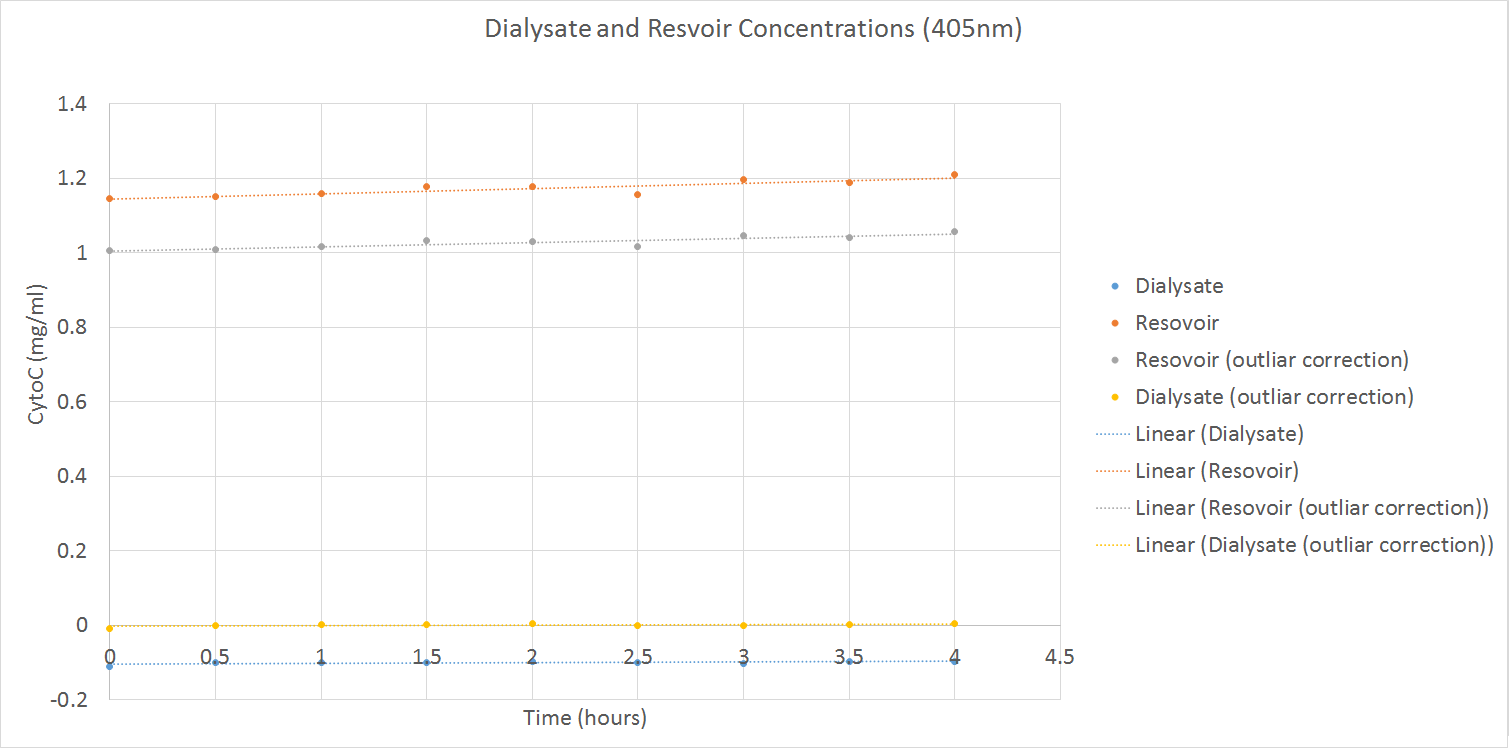
Fig 6. Concentrations of reservoir and dialysate during the dialysate experiment. Adjusted data is included.
Conclusion
There was no detectable dialysis of cytochrome c through the commercial membrane over a four hour period. Dialysate waste concentration did not change over the four hour period, reservoir concentration increased ~5%.
Discussion
The lack of dialysis of cytochrome c is expected. Dialyzer membranes used in current machines are designed to maximize the surface area exposed to both reservoir fluid and dialysate. That membrane area ranges from 1.4-2.4 m^2. In this experiment, an exposed area of only 325 mm^2 was used. In addition, there was pigment change in the dialysate waste after it was passed through the device. This may indicate a component of cytochrome c could pass through the membrane instead of the entire molecule. There was a slight decrease in the volume of the reservoir fluid over time. The flimsy nature of the 325 mm^2 may have contributed to fluctuations in membrane gasket sealing. Future directions include dialysis of urea, incorporation of nanocrystal silicon membranes and microfluidic modeling to compare data sets.
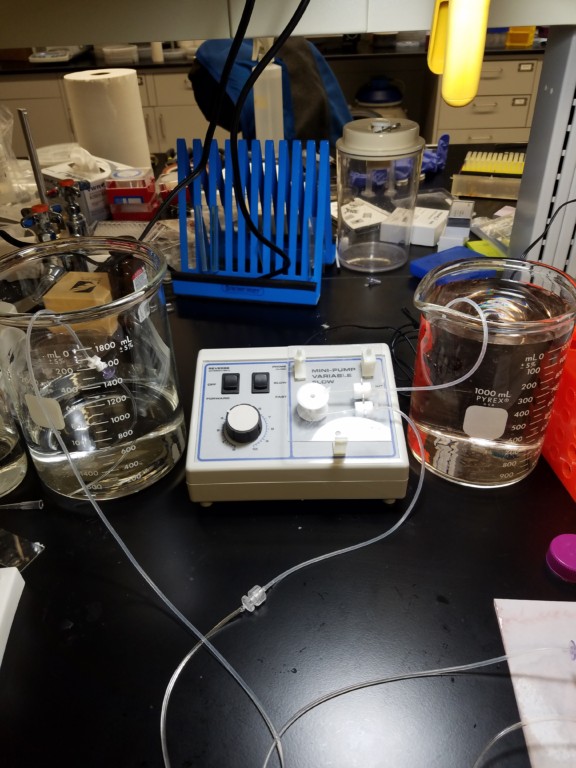
Fig 7. Dialysate and waste dialysate