First Thoughts on ECMO
In preparation for the ICNMM conference next summer (and more immediately, the paper they’ve requested by January) I’ve started thinking about what our membranes can offer extracorporeal membrane oxygenation, or ECMO. This post will begin with some background information that I think is particularly important and progress into what work I’ve done so far on this.
[Be sure to read the update at the bottom]
ECMO is the process of providing cardiac and/or pulmonary assist to a patient by inserting an oxygenator in the middle of an arteriovenous or venovenous fistula. The patient’s blood enters the oxygenator relatively hypoxic (60-70% oxygen saturation) and should leave the device at or very nearly at 100% oxygenation.
ECMO is typically administered with a stream of pure oxygen (~700 mmHg) separated by a membrane from and in counterflow to the blood. The blood is typically passed at a very high flow rate on the order of the patient’s cardiac output (3-6 L/min), in order to best mimic the effects of healthy lungs (pulmonary blood flow is 100% of cardiac output in healthy people.) However, on occasion the primary goal of ECMO is not to assist in oxygenation so much as to allow the patient’s lungs to rest (e.g., to recover from an injury that is being irritated by the motions of breathing.) In this case, a lower flow rate is used (~0.5-1.5 L/min) in order to allow CO2 to more completely leave the blood, as serum CO2 (rather than blood oxygenation) is the direct actuator of breathing rate.
The survival rate of patients on ECMO is abysmal. Complications are plentiful, the most prolific of which is hemorrhaging, which occurs in as much as a third of people receiving the treatment. Hemorrhaging often causes severe morbidities such as kidney failure and stroke, with younger patients at particular risk for brain hemorrhaging. The direct causes of this severe hemorrhaging during ECMO are side effects of the large blood volume and high flow rate of the extracorporeal device: hypertension and hemodilution of clotting factors due to increased circulatory volume, among others.
The vast majority of ECMO treatments are performed on pediatric patients, and neonates in particular. Children pose a special challenge for ECMO devices because in spite of the diminished flow rate requirement (smaller body means lower cardiac output,) it is (apparently) of significant difficulty to design devices with low extracorporeal blood volumes in proportion to a child’s total blood volume. While traditional wisdom prescribes that an extracorporeal blood circuit should not account for any more than 10% of a patient’s total blood volume, pediatric ECMO devices are often twice that size or larger. This is the most obvious place where I have identified a potential application for nanomembranes.
I set out to build a model of blood oxygenation that would enable me to prototype nanomembrane ECMO devices and make predictions of what sort of dimensions would be required. There are, at minimum for a first-order approximation, four types of transport that I need to account for in this model:
- Dissolution of oxygen from the gas phase into the liquid phase
- Diffusion of oxygen within the liquid phase
- Consumption of oxygen and deoxyhemoglobin to form oxygenated hemoglobin by reaction
- Convection of both oxygen and deoxyhemoglobin by blood flow
The most direct way to write these processes together is as a pair of simultaneous partial differential equations:
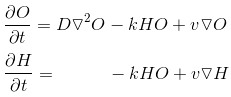
Here, O represents the concentration of oxygen in the blood and H represents the concentration of deoxyhemoglobin. The first term depending on the diffusivity D is diffusion; the second depending on a second-order rate constant k is reaction; and the third depending on the velocity field v is convection.
The hemoglobin has no diffusive term because it is confined within red blood cells, which I am assuming do not diffusive appreciably over the time scales considered here. The rate constant is a complicated value depending on a few parameters including the oxygenation state of the hemoglobin molecule (e.g., the rate of binding of the first oxygen molecule isn’t the same as the rate of binding of the last one) but I have approximated it with an average value of 4 * 10^7 1/(M*s). The diffusivity of oxygen in blood is on the order of 10^-5 cm^2/s.
Because these equations are so difficult to solve analytically (as far as my level of PDE’s prowess is concerned, anyway), I implemented them in COMSOL. I set the source of the flow to 60% oxygenation and the concentration of oxygen at membrane to the solubility of oxygen in blood at 700 mmHg gas pressure, using Henry’s Law. I fixed the volumetric flow rate to an upper-end guess of a neonate’s cardiac output by using a laminar flow simulation and passing the velocity field as ‘v’ to the PDE’s, and then varied the geometry of the system until I found something that achieved >95% oxygenation at the outlet.
One of the things you quickly learn when you start applying numbers to this problem is that blood has a ferocious appetite for oxygen, relative to the rate at which oxygen enters the blood. Many of my first attempts (using devices similar to those that I’ve determined are suitable for hemodialysis) left the blood only marginally more oxygenated than when it entered the device. Because oxygen is consumed so rapidly as it enters the system (instantly as it comes into contact with deoxyhemoglobin, more or less,) the extraordinary advantages offered by thin channels in hemodialysis really don’t cut it here. Instead, I found that thicker channels with slower blood flow velocities tended to be preferable.
I found that one successful design is to incorporate membranes on both sides of the flow (mimicking the advantages of a hollow fiber membrane, to some extent) with membranes of size equal to the area I’ve proposed for dialysis (30-by-30 mm each). This design’s total blood volume (not including tubing, pump, etc.) is a mere 0.45 mL, two orders of magnitude smaller than the leading device currently in use and a tiny fraction of even a premature newborn’s circulatory volume. Similar clearance characteristics are possible with two serial oxygenators with only a single membrane, but this doubles the volume in exchange for an easier fabrication process.

The key assumption I’ve made here is that the rate of oxygen dissolution through the membrane into the blood is so much faster than the rate of its diffusion away from the membrane into the blood, that the oxygen concentration can be assumed to be maintained constant at its solubility next to the membrane on the blood side. This assumption is typical in transport problems involving direct gas-liquid interfaces, and is probably very good in that case; so the question we need to answer is whether or not adding an ultrathin silicon membrane at the interface changes the story. Presumably, adding a thick polymer membrane does change things (otherwise you would expect microliter-scale oxygenators to already exist,) so the next step for me is to look into the validity of this assumption, either experimentally or theoretically.
UPDATE 1/30/16: I’ve come to believe that these conclusions were reached in error. Possibly my mesh size was too large to accurately model the large gradients created by the reaction. My more recent conclusions can be found in my ICNMM paper, “Nanomembrane for Improving Extracorporeal Blood Therapies”.