Long Term Urea Clearance with long term pretreatment
In order to address the fluctuations in the clearance data at the beginning of the long term treatment previous post
The new protocol is as follows:
1. An inspected single slot dialysis chip is clamped into an acrylic fixture holding PDMS ports with glass capillaries.
2. Ethanol is drawn into the device and the connecting flexible tubing with a syringe.
3. A 10-mL syringe, filled with degassed PBS, is placed in a syringe pump (2.9 µL/min) and connected via three way valve to the device.
4. The device is placed in a beaker of PBS with a stir bar with the output tubing directed to the a single .
5. The pump was operated for 35 hours, first pumping the ethanol in the 6 inches of tubing, then the PBS through the device.
6. Anther 10-mL syringe is filled with 30% FBS, 70% PBS, (0.5 mM urea) after degassing.
7. The serum mixture is pumped at 5.6 µL/min with the output going to the fraction collector.
Note that the initial fractions collected will be pure PBS with more serum mixture being introduced later. The fractionator was set to collect 30 minutes of fluid.
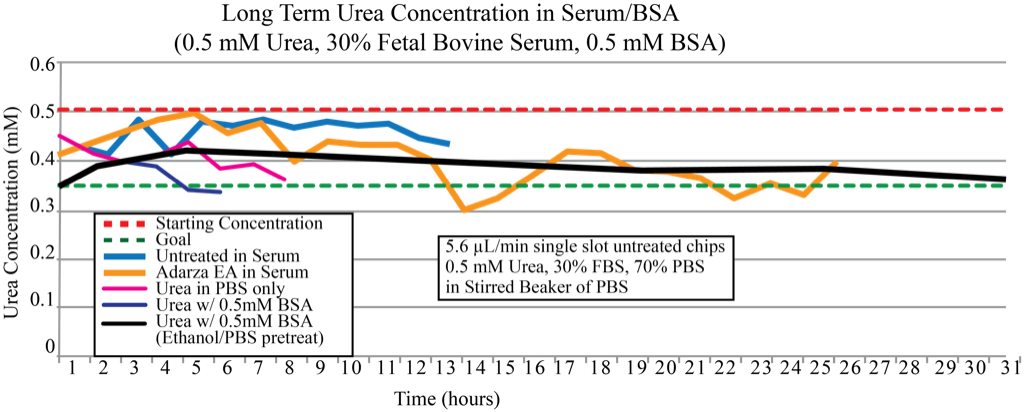
The Black line is the new data. The initial rise in concentration is due to the PBS left in the system which is collected. I’ll calculate when the serum should be through to the fractionator and this will hopefully eliminate that first upwards slope. It is still a mystery why the clearance gets progressively better, but the pre-treatment with ethanol and PBS does eliminate the early fluctuations.
Good progress on the stability!
For the mystery of the steadily increasing clearance, have you thought about the effects of a small pressure differential into the open beaker? If you are forcing fluid into the beaker convectively, you would reduce the effect of diffusion. Over time, this convective flow will slowly clog the membrane with protein, slowing convection, but allowing diffusion of a small molecule like urea, so the observed efficiency would appear to increase.
Alternatively, have you checked the osmolarity of the serum solution vs. the dialysate? IF you have an osmotic imbalance, an osmotic flow could also interfere with urea diffusion. This effect would slowly dissipate as the osmotic balance comes into equilibrium.
These are the only 2 possibilities that come to mind at the moment…