Hemocompatibility Assessment of Microfluidic Extra Corporeal Membrane Oxygenator
Introduction
Risks of extracorporeal membrane oxygenation (ECMO) therapy can be attributed to large membrane areas and blood circuit volumes. These are particularly problematic in neonates with low blood volume. To address this, we are developing a miniaturized prototype microfluidic ECMO using ultrathin highly porous silicone membranes. Hemocompatibility (hemolysis and thrombosis) assessment of geometrical variants of the prototype design have been performed. Thrombosis assessment of the device means, the measurement of how the devices affect the thrombogenic potential of the blood.
Method and Materials
Flow paths and device housings were 3D printed using a stereolithography (SLA) printer. Four geometric variants (baseline, herringbone, reduced gap, and reduced port) of the blood side of a microfluidic oxygenator were fabricated to analyze the blood damage behavior with a reduced volume recirculating circuit driven by a custom-built syringe pump (Fig. 1,2).
Hemolysis Assessment Experiment
Blood was passed 650 times through each device at a flow rate of 100 ml/min and sampled periodically to determine hemolysis (cell-free hemoglobin according to the Cripps method converted to Index of Hemolysis, IH%). The slope of a linear regression between IH% and the number of passes through the device (IH%/pass) was used as a comparative measure of damage and compared to results from a prior numerical model. The hemolysis levels generated from the devices were compared to that of a device-free tubing-only circuit.
The same experiment was replicated with the Silicone Nitride (SiN)membrane material within the blood side and the oxygen side of the device. However, to eliminate the risk of membrane rupture, the membranes had an intact silicon wafer backing as mechanical support. The purpose of this experiment was to see if the membrane material had any effect on hemolysis.
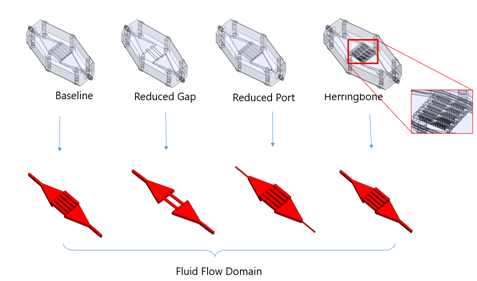
Fig. 1. Four geometrical variants of the microfluidic oxygenator for hemolysis experiments
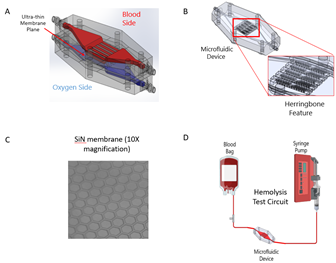
Fig. 2. (A) Microfluidic oxygenator with ultra-thin highly permeable membrane, (B) Blood side of the oxygenator with herringbone features, (C) SiN nanomembrane, (D) Experimental setup of hemolysis experiment. Test circuit with Custom Syringe Pump, Microfluidic Devices, and Blood Bags.
Thrombosis Assessment Experiment
Bovine calf blood citrated with Na Citrate anticoagulant was used for the experiments. 35 ml of bovine blood was flown through the loop 400 to 800 times. 1 ml of bovine blood was sampled before the experiments (0 passes through the device) from the container, at the mid-time point of the experiment (400 passes), and at the end of the experiments (800 passes). To prepare the sample for TEG, the citrated blood sample was mixed with Kaolin and 12.5 ul of CaCl2. The reason for choosing this volume of CaCl2 was, any higher The R time reading was obtained as the marker of thrombogenicity of the devices. Four replicates of the initial blood sample were analyzed before every experimental day to test the repeatability of the results. On one of the experiment days, an Ultra Shearing device (small bore tubing) was also tested to see if highly sheared blood gives a different R reading.
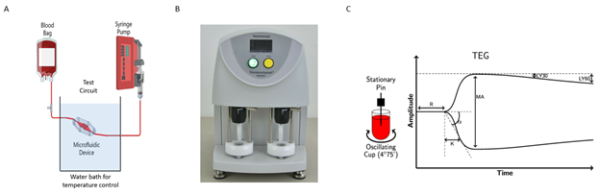
Fig. 3. (A) Experimental setup of thrombosis experiment with water bath temperature control. (B) Thrombo-elastic device: TEG 5000, (C) TEG 5000 output result.
Results
Hemolysis Assessment
The observed hemolysis for all four microfluidic devices was remarkably low (> 0.0003 IH%/pass). A maximum of 3 parts per million of RBCs are damaged by the combined device, tubing, and pump. The incremental damage caused by any of these devices is less than 1 ppm.
Experiments with membrane material showed no significant difference in hemolysis levels when compared to a no-membrane device.
These results are a step in the right direction for the advancement of microfluidic dialyzers and oxygenators, as low sensitivity toward blood damage is a prerequisite for practical implementation in the future.
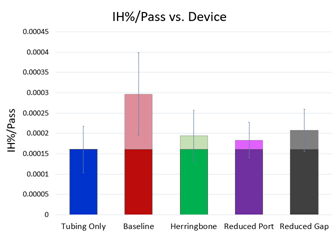
Fig. 4. (A) Overall mean of empirical data comparing IH%/Pass for each device. The lighter shade in each bar represents the device only damage caused by the corresponding device. Error bars represent the standard error of the mean.
Thrombosis Assessment
The results have been summarized in figure 2. It was observed that the R time decreased for the blood that went through the devices when compared to the blood which was sampled from the container (Mann Whitney test, p < 0.05). The Ultra damage device did not show a substantial difference when compared to other devices. From the result it can be concluded, the devices (Baseline & Herringbone) had an effect on the blood thrombogenicity.
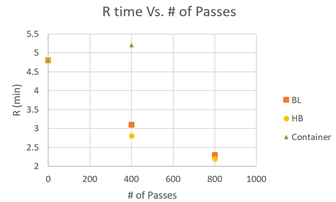
Fig. 5. (A) R time Vs. number of passes for Baseline, Herringbone device and control (container).
Conclusion
To develop the Microfluidic ECMO, hemocompatibility (hemolysis and thrombosis) testing have been performed and promising outcomes were observed for hemolysis experimental cases. For thrombosis assessment it can be concluded, the devices (Baseline & Herringbone) had an effect on the blood thrombogenicity. Further experimentation is required for a conclusive thrombogenicity assessment of the devices. However, the R values of our oxygenator lie within the comparable ranges mentioned in current literature [1].
Reference
- Santos, Jose, Else M. Vedula, Weixuan Lai, Brett C. Isenberg, Diana J. Lewis, Dan Lang, David Sutherland et al. “Toward Development of a Higher Flow Rate Hemocompatible Biomimetic Microfluidic Blood Oxygenator.” Micromachines 12, no. 8 (2021): 888.