ASAIO Conference
June 19
Random Notes
• Blood Stasis is the main cause of thrombosis
• 23 French can access the venous system
• 3 French per mm
• Extracorporal Membrane Oxygenator used in the treatment of Cardiogenic Shock
◦ Use ECMO as a short term mechanical assist device
◦ Peripheral vs. Central venus access – choice
◦ 3L/min is the rate through ECMO
June 20
Left ventricular End-diastolic Pressure-dependent Passive And Active Flow Adjustment Scheme In Continuous-flow Left ventricular Assist Devices
Vakhtang Tchantchaleishvili, MD, University of Rochester, Rochester, NY
Panel
The Cordex SmartcuffTM: A Direct, Calibrated Measurement Of Endothelial Dysfunction
Kathy Magliato, MD, MBA, St. John’s Health Center, Santa Monica, CA
Posters
Development of an Ultra-compact Membrane Oxygenator for New Born Infant
Shohei Nukii, BS, Tokyo Denki University, Tokyo, Japan
• PRIMING volume of conventional devices is 45 ml
• Dropped to 20 ml in this device
• Flow rates ~400 ml/ min. With CO2 transfer and O2 transfer at 20 ml/min
• Use hollow fiber membrane
Utility Operating Method to Achieve Effective veno-venous Extracorporeal Membrane Oxygenation
Konomi Togo, MA, National Cerebral CV Center Research Institute, Osaka, Japan
• Flow rates are 2.5 l/min. Transfer rates are 150 ml/min
• Use PMP membrane
An in vitro System to Replicate Thrombosis in ECMO
Susan Hastings, BS, Georgia Institute of Technology, Atlanta, GA – ASAIOfyi Member
• ECMO has very high rate of complications
• Clotting and hemorrhage
• Clots form at connector step size changes. Clots found mostly on the downstream side of the connectors
Hastings Lecture
The father of rotary heart pumps
11:00-11:30am – ASAIO Hastings Lecture – Serene Stupidity
Richard Wampler, MD, Associate Prof Surgery, Oregon Health Sciences University, Loomis, CA
- Thomas Edison – there are no rules around here we are trying to get things done
- Trust your crazy idea
- Be prepared for soul crushing failures
- Never, never, never give up – Churchill
- Whatever you can do or dream you can. Begin it. Boldness has genius power and magic in it. – Goethe.
My thought: Impeller rotors could be used in our device.
RENAL 3 | VASCULAR ACCESS: INNOVATIvE DEvICES
1:30-3:00pm – Fairchild Room Co-Chairs:
Lalathaksha Kumbar, MD, Henry Ford Hospital, Detroit, MI
Jeffrey Lawson, MD, PhD, Duke University Medical Center, Durham, NC
1:30-1:45pm
Arteriovenous Fistula Eligibility System
Nicholas Franano, MD, Flow Forward Medical Inc, Olathe, KS
1:45-2:00pm
• 6 mm in diameter and 600 ml/min for maturity
• 12 to maturity wall shear stress is the key
• 40-50% fail to mature and are abandoned
• A large group are not eligible because their veins are too small
• Why is AV fistula maturation rate so low
• Nobody knows but these guys have a theory
◦ pulsatile cyclic stretching of the vein wall when attached to the artery
◦ vein wall thickening, smooth muscle response to pulsatile flow – this is called hyperplasia
◦ Poor wall shear stress control –
▸ too low no dilation
▸ too high strip endothelium
• How do we get better flow? Can`t do it with a fistula.
• AFE system dilates veins prior to AVF surgery using controlled, non-pulsatile flow
• Did 2 non-clinical studies (pigs)
• Gets great results
• Providing non-pulsitile flow, in vivo priming to dilate veins before surgery.
• Use pump to prime veins with non-pulsatile flow much faster maturation
• Can use mall veins.
• Not sure what will happen when connection is made, but early fistula loss should be avoided
TvA-FLEx Percutaneous Autogenous Arteriovenous Fistula
William Cohn, MD, Texas Heart Institute, Houston, TX
2:00-2:15pm
• Successful AV fistulas need 2-3 additional procedures DDS
• Non-surgical
• Injects a system to push a couple of catheters into neighboring vein and artery.
• Uses an electrical pulse to fuse the two. Unclear exactly how this works.
• Fistula development and
• Some complications triggering neuromuscular response. Arm moves!
• 28 successful patients and 27 that had useable fistulas at 3 months. A couple of problems. These patients were on dialysis at 3 months and at 6 months.
• Does procedure on brachial vein
Optiflow vascular Anastomosis
Adam Dakin, MBA, Bioconnect Systems Inc, Ambler, PA
2:15-2:30pm
• A connector between the artery and vein
• made of siliconized polyerothene
• fistula first catheter last
• catheters are the second leading cost of death
• failure to mature is the leading problem with fistulas
• 50% probability that you are going to have to do another fistula after 6 months
• Idea is to create a controlled flow conduit
• Adverse remodeling happens around the device. Does not constrict flow. Lumen stays the same size.
• 20% will thrombos during first 6 weeks
• Anastemosis is the name of the junction between artery and vein
• Optiflow Anastemosis
• Published in the journal of vascular access
• Doc says there are similar devices for small vessels. Used in coronary grafts with much smaller flow rates. 60 cc/min. These might be the right thing for us.
▸ Doc says 20% of patients have arteries that are not usable.
NexSite Catheter
Chris Davey, MBA, Marvao Medical Devices Ltd, Galway, Ireland
2:30-2:45pm
• Their are innovations left in the catheter markets
• Known as the `white hose of death`
• infection rates are unacceptably high
• CMS is shifting cost to providers
• CRBSI is the acronym for infection
• Still a population that requires catheters
• What is out there that has worked to reduce CRBSI?
• Rabindrath 2009 meta analysis
◦ Concluded that the antimicrobial coatings don`t work
◦ Management of catheter does help
• Modified catheter cuff
Practical Lifelong vascular Access For Forearm Wearable Artificial Organs
Arnold Lande, MD, Northport Navigable Waters Institution, Northport, MI
2:45-3:00pm
• huge effort on closed loop artificial pancreas
• Since the 1983 whole group has believed cannot access blood over a life time
• Tried to go to subcultaneous tissue. All kinds of problem
• Biostator is a bedside system that has worked since the 80s. Controls glucose levels
• AVF fistula causes the artery going down the arm and larger arteries migrating into the lower arm.
• Vein Fistula Graft is created by a failed AVF that is very stable
• Shows an arm band and futurama character
• aland718@gmail.com from Travers City, MI

Later told me … Blood flow must be above 15 ml/min
Novel Use Of Existing Technology For Better Patient Outcome In Outpatient Hemodialysis Unit
Roshan Patel, MD, Elmhurst Hospital, Elmhurst, NY
RENAL 4 | vASCULAR ACCESS: INNOvATIvE
THERAPEUTICS & MATERIALS
3:45-5:00pm – Fairchild Room Co-Chairs:
Stephen Ash, MD, HemoCleanse, Lafayette, IN
Nicholas Franano, Flow Forward Medical Inc, Olathe, KS
3:45-4:05pm
Immunosuppressive Therapies to Prevent Intimal Hyperplasia
Timmy Lee, MD, University of Alabama, Birmingham, AL
4:05-4:25pm
• Focused on the cell biology and therapies to treat neointimal hyperplasia
• endothelial injury from angioplasty may induce
◦ vascular inflammation
◦ vein is more aggressive response than artery
• looking at drugs that prevent proliferation. paclitaxil. Deliverd at the site where endothelial injury occurs
• studies on treating stenosis have showed poor results
• preventing stenosis
◦ adventitial cells myofibroblasts migrate into the intima
◦ drugs applied directly to adventitia to block activation of fibroblasts and targets downstream
Ension Infection Resistant Surface
Patrick Cahalan, BS, Ension Inc, Cape Coral, FL
4:25-4:45pm
• Best surface is endo/glycocaylx
• Collagen interface to promote tissue integration
• Uses XPS to establish that outer surface is exclusively collagen
Tissue-Engineered vascular Grafts
Jeffrey Lawson, MD, PhD, Duke University Medical Center, Durham, NC
4:45-5:00pm
A Nanofibrous Bioactive Hemodialysis Access Graft
Mauricio Contreras, MD, BIDMC, Boston, MA
June 21
Hemocompatibility Enhancement Of Silicon Nanopore Membranes (SNM) Using Optimized Deposition Of Thin-Film Poly (Sulfobetaine Methacrylate) (pSBMA)
Steven Kim, MD, University of California, San Francisco, CA – ASAIOfyi Member
• 200-600 ml/hr/hG/mm^2 vs 30 for conventional devices
• Zhang et al polymerization to control thickness
• CD62 platelet marker
• PolySMBA
RENAL 6 | ENABLING TECHNOLOGIES FOR WEARABLE
DIALYSIS AND ARTIFICIAL KIDNEY
10:45am-12:00pm – Georgetown West – Concourse Level Co-Chairs:
Stephen Ash, MD, HemoCleanse, Lafayette, IN
William Fissell, MD, Vanderbilt University Medical Center, Nashville, TN
10:45-11:00am
Automated Wearable Artificial Kidney: A Peritoneal Dialysis Approach
Martin Roberts, PhD, University of California, Los Angeles, CA
11:00-11:15am
• Inventor of the REDY sorbant system
• Peritoneal is better because you cannot continuously anticoagulate a patient. Good for about a week (and then it stops being effective?)
• Peritoneal – avoids pumps, anticoatulants, accidental disconnection
• Continuous ambulatory wearable
• Downside – patient intensive, drain peritoneal every 4 hours 7 ml/min flow rates
• Need at least 33 ml/min target 40 ml/min
• Blood tidal PD
Ultrathin Silicon Membranes For Wearable Dialysis
James McGrath, PhD, University of Rochester, Rochester, NY
11:15-11:30am
Nanomaterials To Prevent Membrane Fouling
Baoxia Mi, PhD, University of Maryland, College Park, MD
11:30-11:45am
To reduce fouling
• electrically neutral, smooth,
• polyzwitterion nanobrush
◦ Overall neutral charge
◦ XPS claims to get 100% surface coverage
◦ Doing contact angles, etc.
◦ CBET grant NSF
Dialysate Regeneration With Sorbent Technology
Stephen Ash, MD, HemoCleanse Inc, Lafayette, IN
11:45-12:00pm
• Sorbance has been modeled by Dr. Linda Wine at Perdue University
• Sorbant regeneratino of dialysate for remote, home, acute center, a few liters is all that is needed
• Charcol binds to almost every organic compound Stephen Ash
• Redy column
• Nephology 15 (2010) 406-411
• 2 Kg column
• Redy is uncontrolled dialysis
• 2014 paper in artificial organs on urea clerance
• expers res med devies 4(6) Moving sorbent closer to
• Albumin as a sorbant. Artificial Orgns
• Falkenhagen 2013 plama regeneration
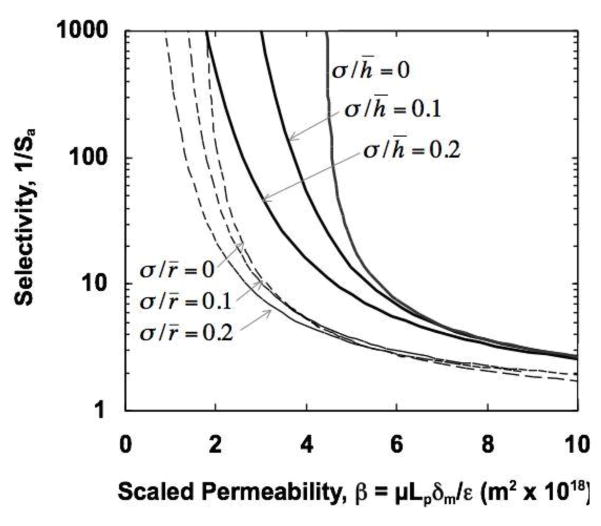
Bioartificial Kidney
William Fissell, MD, Vanderbilt University Medical Center, Nashville, TN
• Medical moonshot. Total implantable. Body doing 100 ml/min
• Elongated slit structures.
• Biomimetic looking at glumerulus structure.
• Double down on elongated slit structure.
• Roy, Fissel Zydney paper JMS makes the case for enhanced permeability at given selection
• 100 nm pore spacing, 7 nm pores, 60 um x 120 um windows
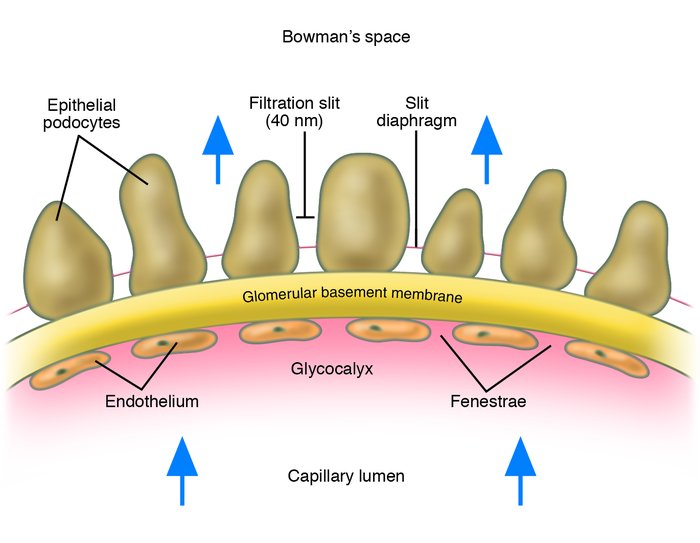
I put a post under “Knowledge” with some images of glomeruli to see the slit structure. No scale bars on these though.
1/3″ diameter catheters? Ouch.
https://trace-bmps.org/blog/knowledge/2014/06/23/what-is-a-glomerulus-and-where-is-it-how-many-are-there?preview=true&preview_id=53285&preview_nonce=fa82e7f394